 Contact Me
Contact MeEndovascular Stent Repair of Abdominal Aneurysm EVAR
 Key hole repair (Endovascular Aortic Aneurysm Repair)
Key hole repair (Endovascular Aortic Aneurysm Repair)
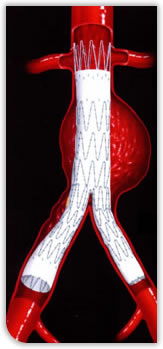
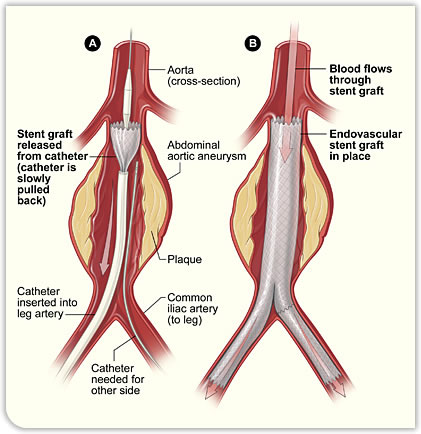
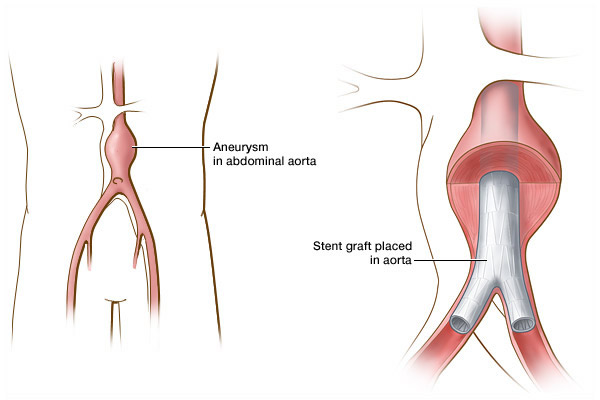
The main alternative approach to keeping high pressure blood away from the inside of the weakened end artery is to do a keyhole repair. This involves inserting a sleeve to line the inside of the aneurysm via the artery in the groin. The same kind of artificial artery used for an open repair is used but it is contained within a narrow flexible tube and has metal springs inside it. The tube with the artificial artery inside it is passed up the inside of the artery and passing up until the weakened part of the artery aneurysm is reached. The sleeve is then opened up and seals off the aneurysm from inside achieving the same thing as in open operation. The seal is achieved by metal springs, which are inside the artificial artery which squeeze it against the inside of the artery, so sealing off the aneurysm. (See diagram).
Picture showing a key hole (Endovascular) aneurysm repair, the material seals off the aneurysm from inside and is held in position with metal springs (you can see one of them poking out of the top)
What are the pros and cons of open vs. endovascular (keyhole repair)?
Both methods have their advantages and disadvantages.
 The
obvious advantage of the keyhole method is that it involves two small cuts in
the groin rather than a large cut on the belly and is a much less major
procedure in terms of the risks of surgery, time taken to recover and so on.
Typically a person having an open repair will be in hospital so about ten days
or so following the surgery and often requires a stay on the intensive care or
high dependency unit. Even once they have been discharged it will take several
months for them to recover fully. The keyhole repair is much more minor
procedure; patients often can go straight back to the ward and usually go home a
few days after the operation. So far it would seem that there is no contest
between an open and a keyhole procedure.
The
obvious advantage of the keyhole method is that it involves two small cuts in
the groin rather than a large cut on the belly and is a much less major
procedure in terms of the risks of surgery, time taken to recover and so on.
Typically a person having an open repair will be in hospital so about ten days
or so following the surgery and often requires a stay on the intensive care or
high dependency unit. Even once they have been discharged it will take several
months for them to recover fully. The keyhole repair is much more minor
procedure; patients often can go straight back to the ward and usually go home a
few days after the operation. So far it would seem that there is no contest
between an open and a keyhole procedure.
Keyhole endovascular repair disadvantages
However there are two major disadvantages to the keyhole procedure as compared with an open repair. Firstly, in order to seal off the aneurysm successfully, a keyhole procedure requires a good length of normal artery above and below the aneurysm so that the graft can successfully seal against the wall of the normal artery in order to make it a blood tight seal and stop any blood reaching the aneurysm. The problem is that for some people the shape of their aneurysm makes this impossible. The commonest reason for this is that the aneurysm goes very close to the arteries which supply the kidneys. In this situation it is impossible to seal off the aneurysm successfully without risking blocking of the blood supply to the kidneys. Other things may also make a keyhole repair difficult or problematic. For example, the arteries may be too narrow to allow the endovascular graft to be passed up from the artery in the groin into the aorta.
 As
a rough guide, about 50 to 60% of aneurysms are anatomically suitable for an
endovascular graft. As technology develops this percentage is increasing.
The other major issue is how well these grafts will work in
the longer terms. In general, once someone has successfully had an open repair,
the aneurysm is very unlikely to cause any further trouble although long term
complications do occur rarely. With keyhole repairs there is more likelihood
that further procedures will be required at some point; For example further
endovascular graft may be needed if the artery the graft was put in becomes
stretched and the graft and artery no longer fit well. Most of these further
procedures can also be done as keyhole procedures, but someone who has had a
keyhole operation is committed to being carefully followed up indefinitely so
that further interventions can be performed should they become necessary. To
some extent, one can regard the keyhole operation as giving a short term benefit
(lower operative risk, quicker postoperative recovery) but there been a
potential downside in terms as a long term effectiveness of the procedure and
likelihood of needing further procedures.
As
a rough guide, about 50 to 60% of aneurysms are anatomically suitable for an
endovascular graft. As technology develops this percentage is increasing.
The other major issue is how well these grafts will work in
the longer terms. In general, once someone has successfully had an open repair,
the aneurysm is very unlikely to cause any further trouble although long term
complications do occur rarely. With keyhole repairs there is more likelihood
that further procedures will be required at some point; For example further
endovascular graft may be needed if the artery the graft was put in becomes
stretched and the graft and artery no longer fit well. Most of these further
procedures can also be done as keyhole procedures, but someone who has had a
keyhole operation is committed to being carefully followed up indefinitely so
that further interventions can be performed should they become necessary. To
some extent, one can regard the keyhole operation as giving a short term benefit
(lower operative risk, quicker postoperative recovery) but there been a
potential downside in terms as a long term effectiveness of the procedure and
likelihood of needing further procedures.
Which operation is right for me?
The first question is whether endovascular (keyhole) repair of your aneurysm is possible. If the shape and size of the aneurysm means that a keyhole procedure is not an option then the only choice is an open repair or not to have it fixed at all. If an endovascular repair is possible, then there are several things to be considered. There is a range of shapes and sizes of aneurysms, which has an effect on how suitable they are for a keyhole repair. Some aneurysms are perfect for keyhole repair, others in others it is clearly impossible but there is some, which are in a grey area in between, which not ideal for a keyhole repair but in whom it could be attempted. There is some research work, which informs this decision. There was a study (the EVAR-2 study) in which patients who are considered so unwell in terms as a general condition such a heart and lung disease etc that they could not be offered an open repair were divided into two groups who were offered either a keyhole repair or else being watched with no repair. It was found that there was no benefit to having the aneurysm repaired in these very high risk groups. I other words, if someone has a number of serious medical problems such as a heart disease or lung disease plus an aneurysm and all of these problems might potentially shorten their life, then trying to fix the aneurysm even with a keyhole repair does not improve their overall life expectancy. To put it bluntly, if you have several medical problems, any one of which may end your life in the near future, then only fixing one of them even with the less invasive method does not improve your overall rate of survival.
What this means is that if the reason for choosing a keyhole repair is because someone is too unwell to have to be capable of having an open repair, then unless the other factors can be corrected as well, it may not be sensible to repair the aneurysm by any method. Another way of looking at it is that if the shape of the aneurysm makes it not very good for an endovascular repair then you are probably better off having an open repair or not having a repair at all.
Another related issue is age and life expectancy. In general, aneurysms affect elderly men who by definition have a relatively limited life expectancy. In this group the long term results of endovascular repair may not be such a factor whereas in somebody who presents with an aneurysm in their 50s and 60s, they may be much more relevant. The issues involved here are complicated and the decision is something, which needs to be carefully considered between the surgeon and the patient and their family and there is no clear right or wrong answer. It is sensible to discuss these issues in detail with your surgeon when deciding whether to have a repair and if so which sort to have.