 Contact Me
Contact MeCarotid surgery for the prevention of stroke
What is a stroke?
 A stroke occurs when the blood supply to the brain is disrupted. This can occur when there is bleeding within the brain (haemorrhagic stroke) or when the blood supply to a part of the brain becomes cut off (ischaemic stroke). The ischaemic type of stroke is by far the commonest and is the sort we are concerned with in the discussion that follows. The blood supply to an area of the brain can be suddenly cut off either because the artery supplying that bit of the brain becomes diseased or because material from somewhere else upstream travels down the artery and blocks it (embolisation). One of the commonest sources of embolisation is disease in the carotid artery. This is the artery that runs in the neck taking blood up to the brain. However, there are other possible sources of embolisation, for example, coming from the heart (atrial fibrillation) or coming from other arteries. The process that causes arteries supplying the brain to fur up (atherosclerosis) is the same one that causes arteries to fur up in the legs, causing pain on walking or arteries to fur up in the heart causing angina and heart attack. See "why do people get arterial disease?"
A stroke occurs when the blood supply to the brain is disrupted. This can occur when there is bleeding within the brain (haemorrhagic stroke) or when the blood supply to a part of the brain becomes cut off (ischaemic stroke). The ischaemic type of stroke is by far the commonest and is the sort we are concerned with in the discussion that follows. The blood supply to an area of the brain can be suddenly cut off either because the artery supplying that bit of the brain becomes diseased or because material from somewhere else upstream travels down the artery and blocks it (embolisation). One of the commonest sources of embolisation is disease in the carotid artery. This is the artery that runs in the neck taking blood up to the brain. However, there are other possible sources of embolisation, for example, coming from the heart (atrial fibrillation) or coming from other arteries. The process that causes arteries supplying the brain to fur up (atherosclerosis) is the same one that causes arteries to fur up in the legs, causing pain on walking or arteries to fur up in the heart causing angina and heart attack. See "why do people get arterial disease?"
How does arterial disease in the carotid arteries cause a stroke?
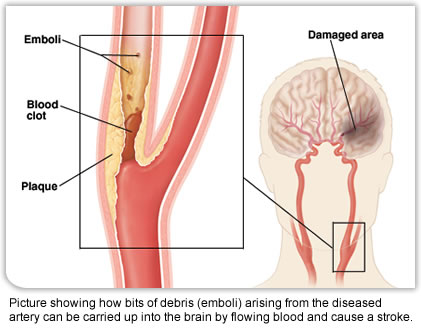 The carotid artery divides into two in the upper part of the neck. One branch, the external carotid, gives off lots of branches that supply the face, tongue and other areas. The other, the internal carotid takes blood up to the brain. Arterial disease is particularly prone to occur where arteries branch and it is quite common for arterial disease to build up around where the artery divides into two and to narrow the start of the internal carotid artery. The narrowing of the internal carotid artery reduces the amount of blood getting through but this does not usually cause symptoms because there are other routes of supply, for example, the carotid artery on the other side or the vertebral arteries which supply the back of the brain and all these arteries join up inside the skull so that if one of them becomes narrowed, the others can usually take over the supply, so that furring up of the arteries can gradually build up over many years without necessarily causing any symptoms. However, sometimes the area of furring up of the artery can become unstable and the surface of it splits open. The blood circulating in the artery then tends to clot onto this raw surface and bits of blood and debris from the furred up artery can then break off and be carried in the flowing blood up into the brain (embolisation). How far they get depends on how large the particles are but as the arteries go up into the brain they divide into smaller and smaller branches, a bit like a tree dividing into branches, small branches, twigs etc. Sooner or later the arteries will not be big enough to allow the debris to keep moving and will become blocked. When this happens, the area of the brain supplied by that particular blood vessel will have its blood supply interrupted and stop working properly. When this process suddenly cuts off the blood supply to a part of the brain a stroke occurs.
The carotid artery divides into two in the upper part of the neck. One branch, the external carotid, gives off lots of branches that supply the face, tongue and other areas. The other, the internal carotid takes blood up to the brain. Arterial disease is particularly prone to occur where arteries branch and it is quite common for arterial disease to build up around where the artery divides into two and to narrow the start of the internal carotid artery. The narrowing of the internal carotid artery reduces the amount of blood getting through but this does not usually cause symptoms because there are other routes of supply, for example, the carotid artery on the other side or the vertebral arteries which supply the back of the brain and all these arteries join up inside the skull so that if one of them becomes narrowed, the others can usually take over the supply, so that furring up of the arteries can gradually build up over many years without necessarily causing any symptoms. However, sometimes the area of furring up of the artery can become unstable and the surface of it splits open. The blood circulating in the artery then tends to clot onto this raw surface and bits of blood and debris from the furred up artery can then break off and be carried in the flowing blood up into the brain (embolisation). How far they get depends on how large the particles are but as the arteries go up into the brain they divide into smaller and smaller branches, a bit like a tree dividing into branches, small branches, twigs etc. Sooner or later the arteries will not be big enough to allow the debris to keep moving and will become blocked. When this happens, the area of the brain supplied by that particular blood vessel will have its blood supply interrupted and stop working properly. When this process suddenly cuts off the blood supply to a part of the brain a stroke occurs.
What symptoms does a stroke cause?
The symptoms resulting from a stroke depend on which area of the brain is affected and how large a part of the brain is deprived of its blood supply. For example if the part of the brain controlling movement of the arm becomes affected then the person's arm may become weak or paralysed. If the part of the brain controlling speech is affected they may be unable to speak or find it difficult to find the correct words. It is important to bear in mind that the brain is essentially divided into two halves, the left and the right. The right side of the brain controls the left side of the body and vice versa. So, for example, if an area on the right side of the brain suddenly loses its blood supply someone may find that they are unable to move their left leg and arm and lose sensation. Or if a slightly different area is affected they may find the left side of their face becomes droopy. The point is that the symptoms occur down one side only. So, for example, it would be perfectly common for somebody to lose use of their leg and their arm on one side but it would not be common for somebody to suddenly find that both their legs did not work. The point of a stroke is that sensation or power is lost as opposed to having funny sensations or abnormal movements. The severity of a stroke is extremely variable. On the one hand a really severe stroke may cause very profound disability, loss of consciousness and even death. On the other hand a minor stroke may recover completely with no signs that it has ever happened. In general the process of recovery from a stroke can take quite a long time because part of the recovery consists of areas of the brain that are next to the damaged one learning how to take over the job that was previously done by the damaged part. In other words, even though a part of the brain remains permanently damaged the function that it previously provided may recover.
What is a mini stroke? (Transient ischaemic attack (TIA))
Obviously, the problem with a stroke is that the first time someone realises they are at risk of one may be the time when they have a very severe stroke which leaves them with a severe disability and by which time the damage is done. However, sometimes people will have mini strokes. These are essentially similar to a stroke as described above but only last a very short period of time and recover completely often within a few minutes or so. The importance of these is that they are early warning signs that people are at a risk of having a (proper) stroke and that they provide a chance to take action to prevent a more serious stroke occurring. About 25% of people who have a stroke will, if asked, describe having had mini strokes prior to this. Unfortunately, because the symptoms recover very quickly people often do not recognise the importance of the problem and do not want to bother their doctor or make a fuss. If they do go and see their doctor there is usually nothing to find on physical examination as everything has recovered and unfortunately the combination of these factors means that there are often delays in properly assessing people who have had mini strokes. This is important because the presence of a mini stroke is a sign that the arterial disease causing the problem is likely to have become unstable and that further bits of debris (emboli) are likely to continue to travel up into the brain. Often the time between the warning mini stroke and a full-blown stroke is quite short and it is therefore important to take a mini stroke seriously and get it assessed urgently. Once again, the signs of a mini stroke come on suddenly, affect one side of the body rather than both arms or both legs and cause loss of power or loss of sensation, sometimes difficulty in speaking, drooping of the face etc. They do not cause loss of consciousness, feeling generally weak or funny or other vague symptoms. The symptoms recover fully and often they may only last a few minutes or sometimes a little longer. Sometimes people notice the weakness when they drop something, my favourite was "my cigarette just fell out of my hand". One particular type of mini stroke occurs when the debris goes into the artery taking blood to the eye instead of into the brain. When this happens people will notice that they suddenly loose vision in the affected eye "like a curtain coming down" because only one eye is affected the vision in the other eye remains perfectly normal. Then after a short space of time the vision returns to normal.
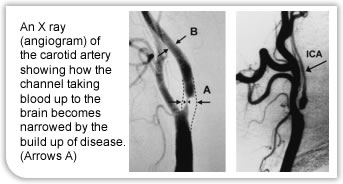 People who have a stroke require emergency assessment by a stroke physician. Modern treatments mean that sometimes, if help is provided rapidly, the blood supply to the injured brain can be restored with recovery of the brain but only if this is done within a few hours of the onset of stroke (thrombolysis). People who have a mini stroke (TIA) also require urgent assessment although not necessarily hospital admission. Stroke physicians increasingly provide rapid access service often six or seven days a week where anyone who has a suspected TIA can be assessed and investigated and treatment started. Treatment consists of starting low dose Aspirin which makes the blood less prone to form emboli, controlling blood pressure, being on cholesterol tablets which help stabilise the furred up areas of artery as well as lowering cholesterol and also imaging of the carotid. People with heart dysrhythmia (atrial fibrillation) causing a stroke will require anti-coagulation. People also have imaging of their carotid arteries and if this shows that there is a tight narrowing of the carotid artery that is thought to be the source of the stroke or mini stroke then this will require treatment.
People who have a stroke require emergency assessment by a stroke physician. Modern treatments mean that sometimes, if help is provided rapidly, the blood supply to the injured brain can be restored with recovery of the brain but only if this is done within a few hours of the onset of stroke (thrombolysis). People who have a mini stroke (TIA) also require urgent assessment although not necessarily hospital admission. Stroke physicians increasingly provide rapid access service often six or seven days a week where anyone who has a suspected TIA can be assessed and investigated and treatment started. Treatment consists of starting low dose Aspirin which makes the blood less prone to form emboli, controlling blood pressure, being on cholesterol tablets which help stabilise the furred up areas of artery as well as lowering cholesterol and also imaging of the carotid. People with heart dysrhythmia (atrial fibrillation) causing a stroke will require anti-coagulation. People also have imaging of their carotid arteries and if this shows that there is a tight narrowing of the carotid artery that is thought to be the source of the stroke or mini stroke then this will require treatment.
How is the carotid artery treated?
There is good evidence from large randomised controlled trials (where half the people had surgery plus medical treatment and the other half just had medical treatment) that carotid endarterectomy substantially reduces the risk of stroke in patients with symptoms arising from disease in the carotid artery. This is not done as an alternative to medical treatment such as cholesterol lowering tablets and so on but in addition. So everyone should have the best medical management of their problem, stop smoking etc. But in addition if someone has symptoms arising from a narrow carotid artery they should be considered for carotid surgery.